
Polycystic ovaries
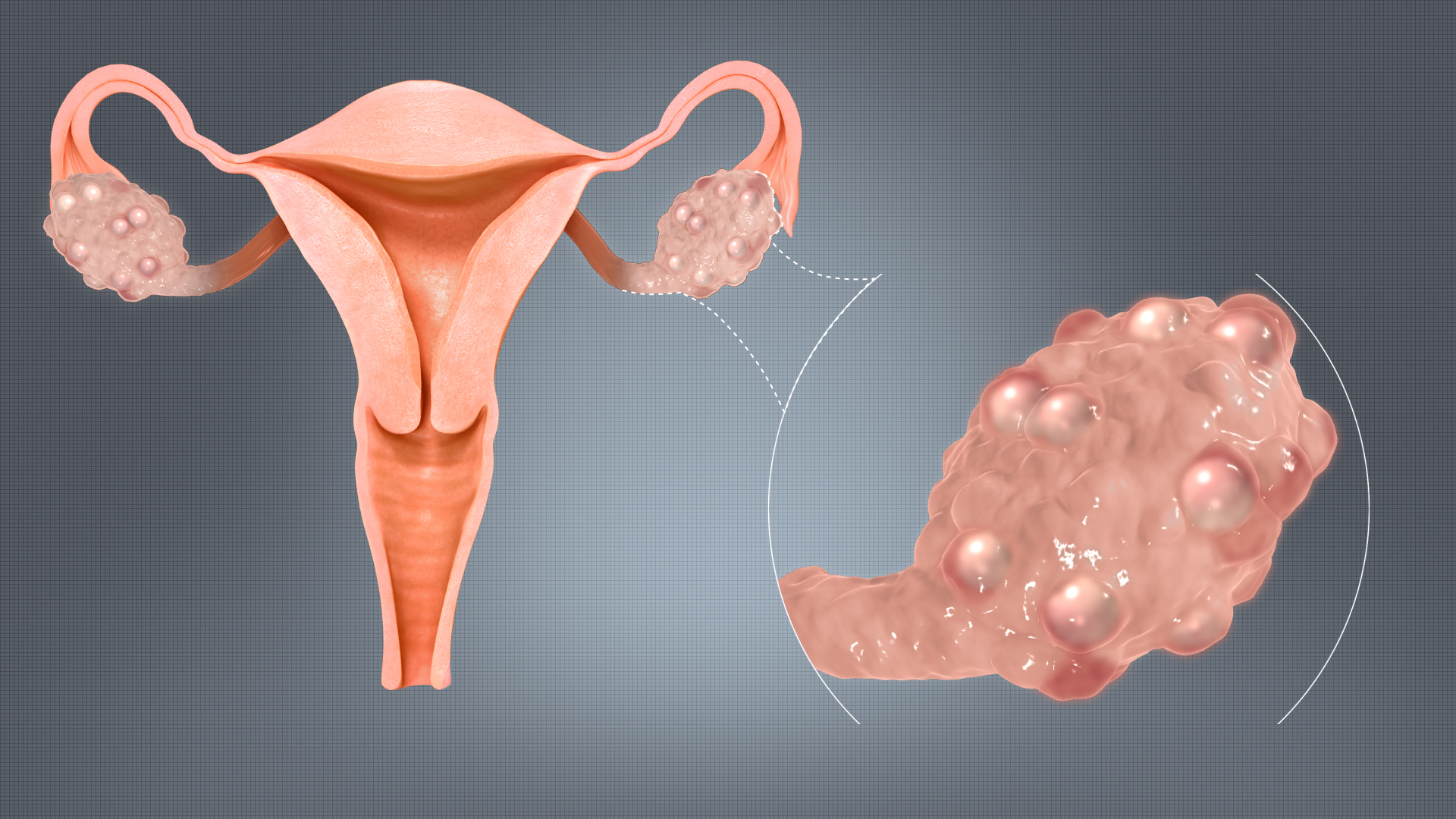
Polycystic Ovaries (Poly-multiple, cystic-fluid filled sacs) are a type of ovaries which are bulky and show numerous tiny follicles wrongly called as cysts.
About 3.7 to 22.5% of women in the reproductive age group face the problem of polycystic ovaries which is characterized by hormonal imbalance, irregular menstrual cycles and excess of male hormone (androgen ) levels.
Women with polycystic ovaries might have excess hair growth over face and body. They might have difficulty in conceiving due to irregular cycles.
Most women find it difficult to keep their weight under control due to insulin resistance which is commonly seen in women with polycystic ovaries.
The mainstay of treatment is a low calorie diet and regular exercise in women who are not interested in child-bearing which itself can make their cycles regular without medication.
Some women having polycystic ovaries might have regular menstrual cycles and some might not have facial hair or acne.The signs and symptoms depend upon the high androgen or male hormone levels and peripheral insulin resistance.
Women who are trying to conceive should meet a fertility specialist. They usually need ovulation induction or medication to induce ovulation.
Ovulation induction with timed intercourse
In this treatment women are asked to come on day 2 or day 3 of periods. They are given some medication which help development of eggs. They are asked to follow up for follicular monitoring sonography in which egg development is assessed. When the size of the egg reaches 18-20 mm size, HCG injection is given to trigger ovulation and the couple is advised to have intercourse the next two days.
Ovulation induction and IUI (Intrauterine insemination)
When 3-4 cycles of timed intercourse fail, then patient is advised IUI treatment in which washed semen sample is inserted inside the uterine cavity around the time of ovulation.The pre-requisites for IUI are patent one or both fallopian tubes.
The treatment starts on the second or third day of periods. The woman is asked to come for a sonography after which some medications are started which help development of egg or follicle. The lady is asked to come for follow up for follicular monitoring. In this we monitor the development of the egg or the follicle till it grows to a size of 18-20mm size. At the same time endometrial lining is also measured which should be ideally more than 7mm around the time of ovulation. Then a HCG injection is given to trigger ovulation.
IUI is done between 36-40 hours after the HCG injection. The husband is advised to abstain from sexual intercourse for 2-3 days prior to IUI. The lady undergoes a sonography to check for ovulation. Semen sample is collected and then processed in the laboratory. Best motile sperms are separated and then inserted inside the uterine cavity with the help of a thin catheter. The procedure is painless.
After the procedure, the lady is asked to lie down and rest for 10-15 minutes. Then she is advised to use progesterone vaginal capsules for 15 days. She is asked to follow up after 15 days with a urine pregnancy test report.
The success rate of IUI is about 10-15%.
IVF ( In-vitro fertilization)
When 2-3 cycles of IUI fail then IVF is advised. Patients of Polycystic ovaries might have poor oocyte quality.
IVF or test tube baby treatment is a procedure where embryos are developed outside the body (In-Vitro) and then transferred back to the uterus.
IVF is advised in
Women having Fallopian tube blocks
- In men with severely low sperm count and motility
- In couples where other treatment options have failed
- In women with low egg count
- In cases of endometriosis, etc
What are the steps involved?
- Once IVF treatment is advised, couples are thoroughly counseled regarding the success rates of IVF
- One month prior to starting IVF, we advise certain blood tests to both and start supplements for vitamin deficiencies and treat infections if any.
- IVF injections start on day 2 or day 3 of periods.
- A baseline sonography is done and injection dose is decided. These injections are hormone injections and are continued for about 10-12 days.
- Sonography is done on alternate days starting from 5th or 6th day of periods.
- Once the size of the follicles reaches 18=20 mm on sonography, trigger injection for ovulation is given and 34-35 hours later egg retreival is done.
- On the day of egg retreival the woman will be called for admission in the hospital in the morning on empty stomach. Egg retreival or Ovum pick up is done under short general anesthesia.
- Patient is discharged 2-3 hours after the procedure. The status of embryos is informed to the couple after 3-5 days.
- Depending upon the case we decide to go for fresh embryo transfer or frozen embryo transfer. In frozen embryo transfer, the embryos are frozen on day 3 or day 5 after ovum pickup.
- The next month when embryo transfer is decided, the woman is called on day 2 or day3 or periods. She is started on medicines to grow the endometrial lining. She is asked for follow on 10th to 12 th day of periods and endometrial thickness is assessed and embryo transfer date is decided.
- On the day of embryo transfer patient is asked to come after breakfast to the hospital. There is no anesthesia given for this procedure. She is asked to keep her urinary bladder full. Embryo transfer is done under sonography guidance. Patient is advised medications for 15 days and asked to do a pregnancy test after 15 days.
- There is no need of bed rest after embryo transfer. You can resume with your routine work after embryo transfer.